Establishing a tertiary care cancer hospital in a developing country: The story of the Shaukat Khanum Memorial Cancer Hospital and Research Center
Professor Nausherwan K Burki, Professor of Medicine, University of Connecticut Health Center, USA; Chief Medical Advisor and Member, Board of Governors, Shaukat Khanum Memorial Cancer Hospital and Research Center, Pakistan
Professor Nausherwan K Burki writes: A first-hand account of establishing a tertiary care cancer hospital in Pakistan, a low- and middle-income country, and the decision-making and challenges behind this. The article looks at how the concept was arrived at, funding concerns, how the hospital was to be administered, the medical staffing of the hospital at all levels and the how the medical services were organized to provide the diagnostic and therapeutic functions, as well as patient care and information. Finally, the article touches on research and the future for the hospital.
Modern cancer care requires a highly trained workforce, sophisticated equipment and facilities, expensive drugs and public awareness. It is not surprising, therefore, that poorer countries lag far behind advanced, developed countries in providing adequate care – diagnostic, therapeutic or palliative – for cancer patients.
Until the early 1990s, Pakistan had no organized focus on cancer patients, even though the country has highly trained physicians and surgeons. Diagnostic equipment was lacking, very few standard chemotherapy drugs were in use and cancer treatment was provided in the general wards of general hospitals by non-specialist physicians and surgeons. It was in this vacuum that a tragedy brought Imran Khan to the cancer scene. In 1990, Imran was an international cricketing celebrity, having captained the Oxford University cricket team and the Pakistan cricket teams; in the same year, his mother died of cancer and he was horrified by the lack of adequate cancer care and palliation that she received. Realizing that if the level of care for someone who could fully afford it was so poor, the care given to the vast majority of Pakistanis who could not afford it must be even worse, Imran determined to build a tertiary care cancer hospital, named for his mother, the Shaukat Khanum Memorial Cancer Hospital and Research Centre, in Lahore, Pakistan, as a model for Pakistan. Because of his cricketing celebrity status, donations began to pour in, but he was not sure where to start.
In 1990, he approached me for assistance in developing the project, while I was a Professor of Medicine at the University of Kentucky in the United States. We agreed on four things – it would be a non-profit charitable institution, it would strive to provide the best, most advanced diagnostics and treatment for cancer, with free or subsidized treatment to all cancer patients who could not afford it, and there would be no direct government involvement.
To develop a master plan for a tertiary care, state-of-the-art, cancer institution in a developing country was a daunting task. No reliable statistics on cancer incidence in Pakistan were available in 1990, concepts of modern hospital management did not exist in the country, nursing training had not kept up with modern trends and there was a dire shortage of trained ancillary health staff. Thus I was presented with a tabula rasa to develop what would be a unique experiment in the country.
I was fortunate when I advertised for a hospital design architectural firm in finding Messrs Arrasmith, Judd, and Rapp of Louisville; their principal, Graham Rapp, was well-versed in hospital design and in working overseas, having designed and built a hospital in Turkey. Most importantly, since our funds were very limited, Mr Rapp stated that fees were not a major concern. I am very pleased to say that the firm has been working with us ever since, and is currently designing our new hospitals in other cities. With this architectural firm, and in discussions with a wide array of friends and experts, we developed a master plan. Not knowing the cancer incidence in the country, one had to pick figures and projections out of the air: recognizing that modern cancer treatment is primarily outpatient based, I projected that in the first year we would have 25,000 outpatient visits and planned accordingly. The master plan was in three phases – starting with 60 inpatient beds with all ancillary services and increasing the inpatient beds to 250 by the end of 10 years. In the event, the timeline was too optimistic, and the phases have stretched out over 20 years, rather than the proposed 10 years. The hospital has been built according to the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) standards and United States’ hospital building codes. Hospital building codes are foreign to most doctors and were to me as a clinician/research worker; over the last 20 years in my role of developing and overseeing this hospital, I have learnt an enormous amount. The Shaukat Khanum Memorial Cancer Hospital opened its doors to patients in December 1994, even while some of the construction work had not been completed.
A major problem in developing such an institution in Pakistan, or any developing nation for that matter, is the absence of supporting facilities – we could not simply rely on available diagnostic and specialty services in the community or region; there were no trained oncologists, adult or paediatric, intensivists, cytopathologists, etc. In 1990, there was no MRI machine in the region; medical radioisotopes and blood products were generally not available. We were therefore constrained to develop virtually all the necessary diagnostic and treatment infrastructure within the institution.
Financial concerns
The hospital concept was based entirely on donations, since it had been decided that no government involvement would be allowed to avoid bureaucratic or political interference. It was a great surprise, and very heartening, that the Pakistani public, both within and outside Pakistan, has responded enthusiastically, in no small part because of the credibility of Imran Khan and his celebrity status. Imran worked tirelessly soliciting funds around the country and abroad, and people responded enthusiastically. These donations have continued and indeed increased over the years, with publicity campaigns and fundraisers: currently 56% of the hospital budget comes from donations.
Administration
Given the absence in Pakistan of trained staff familiar with modern hospital administration, we decided from the outset that in the initial stages a hospital administrator trained and working in the United States’ would be required. Hospital administrators working in the United Kingdom’s NHS in 1990 were not considered ideal, since most had no experience of running a freestanding, non-profit, nongovernment hospital. Accordingly, the first two hospital administrators were from the United States’. These Hospital Directors recruited local staff for the different administrative functions, some of which had never existed or were rudimentary in the regional hospitals – materials management, management information systems, facilities management, central sterile supply and laundry department, etc. Many of the local staff underwent on the job training and today are highly accomplished in their various administrative fields.
In the first year that the hospital opened, I took a sabbatical from my university and ran the hospital as CEO for 14 months. This allowed me to put in place certain procedures, which are now set in stone. Today, 25 years later, the hospital runs smoothly and efficiently due in large part to these workers.
Nursing
At the outset, we noted that nursing training and nursing procedures appeared to be petrified in the 1950s and if the hospital was to function at international levels, it was essential to improve nursing services and bring them up to modern standards. Accordingly, I determined to initially have a Nursing Director from Europe or the United States’, who would develop a cadre of nurses to train the local nurses. The Nursing Director, Barbara Messer, from California, recruited a small group of nurses from the United Kingdom, Ireland and South Africa who formed a core for training and supervising locally recruited nurses. A number of highly-trained nurses were recruited from the Phillipines by Ms Messer for nurse manager positions in crucial areas of the hospital – the operating suites, the intensive care unit, the chemotherapy unit, etc. This core group developed a re-training programme, consisting of class work, didactic lectures and hands-on bedside training for the recruited nurses. A diploma programme for oncology nursing – the first in the Middle East/South Asia region – was instituted. The result of this planning and training is that the hospital now has highly-trained Pakistani nurse administrators and nursing services comparable to any hospital in the world; in addition, the hospital has the only group of trained oncology nurses in the region.
Medical services
It was decided at the outset to recruit physicians who were currently trained in Europe or the United States’ to bring the latest techniques and concepts to cancer care at the hospital. While we advertised for all physicians of any nationality, Pakistan is fortunate in having a large diaspora of highly-trained physicians. It is also a curious fact that virtually all members of this diaspora yearn to return to their homeland, especially when their children come of school age. Thus, I was able to recruit a number of physicians who had just completed their fellowship specialty training in various fields in the United States, Britain and Ireland. Their fresh knowledge was a boon, but their lack of administrative experience needed to be nurtured. It is very heartening that now, 25 years later, they form a mature, experienced group, responsible for excellent results at the hospital. In this regard, Dr Faisal Sultan and Dr Aasim Yusuf are to be singled out for exemplary service. Dr Faisal Sultan, an infectious disease specialist, has been the CEO for more than 15 years and Dr Aasim Yousuf, a gastroenterologist, has been the Medical Director and now Chief Medical Officer for the same time. They have guided the hospital to Joint Commission accreditation (in 2018) and they continue to oversee excellence at the Hospitals of the Shaukat Khanum Trust.
Initially, I had hoped that certain specialty services – neurosurgery, nephrology, orthopaedic surgery, urology, etc., could be provided by part-time visiting surgeons and physicians from the community. However, this turned out to be impractical and now the hospital has a full complement of full-time medical and surgical specialties.
Diagnostic services
Laboratory and imaging services had to be developed from scratch and were fortunate in being able to recruit accomplished pathologists and radiologists. In 1994, cytology services did not exist in Pakistan; on hospital opening day, an Australian tourist happened to be present. It turned out that she was a cytology technician and she agreed to stay on and train our technicians. She stayed with us for one year and established the cytology services. Molecular biology and genetic services became available with the development of our research services (see below).
The hospital installed the first MRI machine in the region in 1994. Subsequently, we installed the first (and still the only) PET scanning unit in the region. Unlike in advanced, developed countries, we were forced to install our own cyclotron for manufacture of radioisotopes because of non-availability and the short half-life of radioisotopes.
Today, the hospital has a full complement of diagnostic laboratory and imaging services, which include CAT scanning, ultrasound facilities, PET/CT scanning and nuclear medicine. The pathology laboratory subscribes to the College of American Pathologists (CAP) quality control programme to ensure accurate results.
Therapeutic services
As cancer treatment takes three forms – chemo- or immunotherapy, surgery, and radiation therapy – all three modalities needed to be available.
The hospital provides adult and paediatric oncology services, with a full backup of associated specialties – intensive care, pulmonary medicine, gastroenterology, infectious diseases, etc.
Chemotherapy:
The Hospital plan includes a 30-bed chemotherapy bay (20 adult and 10 paediatric beds), plus a further 10 beds on an inpatient floor, providing 130 chemotherapy and transfusions daily. Further expansion of this area is in progress. When the hospital opened, the majority of standard chemotherapeutic drugs were not available in Pakistan. Over time, after negotiations with multinational pharmaceutical manufacturers, these drugs have become available and now the latest, most effective drugs are provided to the patients.
Radiation medicine:
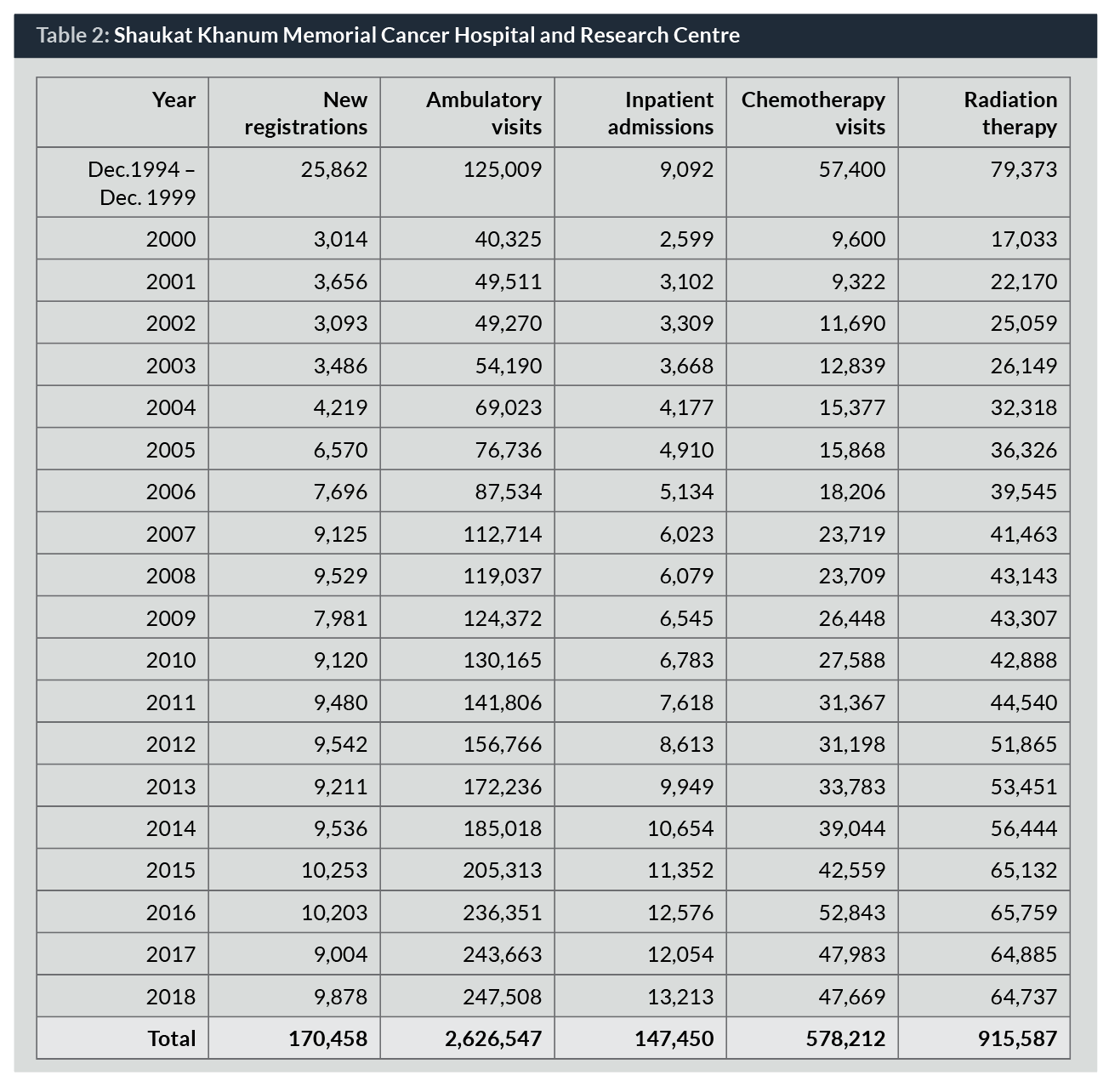
At the time of planning the hospital, all radiation facilities in Pakistan were under the control of the Federal Atomic Energy Commission (AEC), and the only radiation therapy units that existed were in freestanding government-run facilities, many with outdated equipment. The Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, became the first hospital to install radiation equipment, approved by the AEC. Currently, with five linear accelerators, radiation treatment is provided to 207 patients daily (Table 2).
Palliative care:
The concept of palliative care did not previously exist in Pakistan. A palliative care unit was established at the hospital for cancer patients and provides appropriate care to these patients.
Hospital pharmacy and blood bank:
The concept of an integrated hospital pharmacy was a foreign concept in Pakistan. The Shaukat Khanum Memorial Cancer Hospital & Research Center was the first institution to establish a proper hospital pharmacy, with pharmaceutical advice on drug interactions, dosages and toxicity available to the doctors.
Similarly, at the time of establishing the hospital, blood product usage in the country was very basic, with most patients receiving whole blood when necessary. The hospital established its own blood bank and brought in the concept of blood products and donor testing for hepatitis and HIV, etc. This has now been emulated in many institutions in Pakistan.
Hospital information services
Over the years, the hospital has developed its own comprehensive software, with a Hospital Information System department of 15 software engineers. The hospital is now essentially paperless. This system has been provided free of cost to government hospitals, particularly in the Northern province of Khyber Pakhtunkhwa.
Patient care
At the outset, given that this was to be a non-profit hospital dependent on donations from the public, two concepts were enforced:
The most important of these is the concept of patient registration based on first come, first served. In developing countries like Pakistan, rules are elastic and the wealthy and influential usually manage to override them to their own benefit. However, we made this a rigid rule, and because it was apparent that I would not budge from this rule, there were very few attempts to circumvent this, including by some from the highest in the land, and today the registration system functions smoothly on this basis.
A second absolute rule is that once a patient is registered into the system there is no distinction in services provided to non-paying versus full-paying patients. The outpatient facilities, the inpatient rooms and facilities, the chemotherapy and diagnostic services are all equal for all patients. In fact, inpatients in the 2-bed rooms (all the inpatient rooms are 2-bed rooms) are frequently completely unaware of the paying status of their companion patient.
In this regard, there were some difficult moral decisions to be made. Since the hospital was predicated on providing cancer treatment regardless of the ability of the patient to pay, it became clear in the first year that we would run out of funds.
The oncologists were therefore requested to decide at what stage of a given cancer, treatment becomes palliative rather than curative, at which point only palliative care would be provided. This was a difficult decision for the oncologists, since by training it is their wont to continue maximum treatment to the end. However, they agreed and this policy was instituted.
This brought another dilemma: the fully paying patients demanded to continue treatment with certain expensive drugs, which they could afford, despite explanations of the advanced stage of their cancer and the long-term futility of the use of these drugs. Was it morally justified to withhold treatment with drugs (that were only available in the hospital pharmacy having been directly imported) that the patient could afford and that might have some temporary benefit or provide peace of mind? This dilemma brought a major shift in hospital function which, in the long run, has been very helpful: patients who are willing to pay the full cost of treatment are registered separately; however, the criteria for admission into the system remains the same for them as for the indigent patients. Once they are admitted into the system for treatment, no distinction is made between them and the indigent patients in terms of diagnosis, treatment or facilities.
A second dilemma surfaced early: as the reputation of the hospital and the quality of its laboratory and diagnostic services spread, many non-cancer patients wanted to use these services. At first, it was felt that since all the donations had been made for cancer treatment, non-cancer patients could not be entertained. However, two considerations came to the fore: it was not considered morally acceptable to withhold diagnostic services from patients willing to pay the full charge, especially since we had excess capacity and in some cases, for example MRI services, the only diagnostic capability in the region. The income from these services would help to provide better care for the cancer patients. Therefore, the diagnostic laboratory and imaging services were opened to non-cancer patients with the proviso that this would in no case jeopardise the availability or timeliness of these services for the cancer patients. The same considerations were then applied to the available medical expertise and the medical staff were permitted to see non-cancer patients on the same basis.
These decisions have led to the opening of more than 200 diagnostic collection centers around the country, where patients can have blood or urine samples taken and sent to the main laboratory, and in the majority of cases have the results available to them on the web the same day. This is now not only a significant medical resource to the country, but a significant source of funds for the hospital.
We had projected that in the first year there would be 25,000 outpatient visits; in the event there were 23,500.
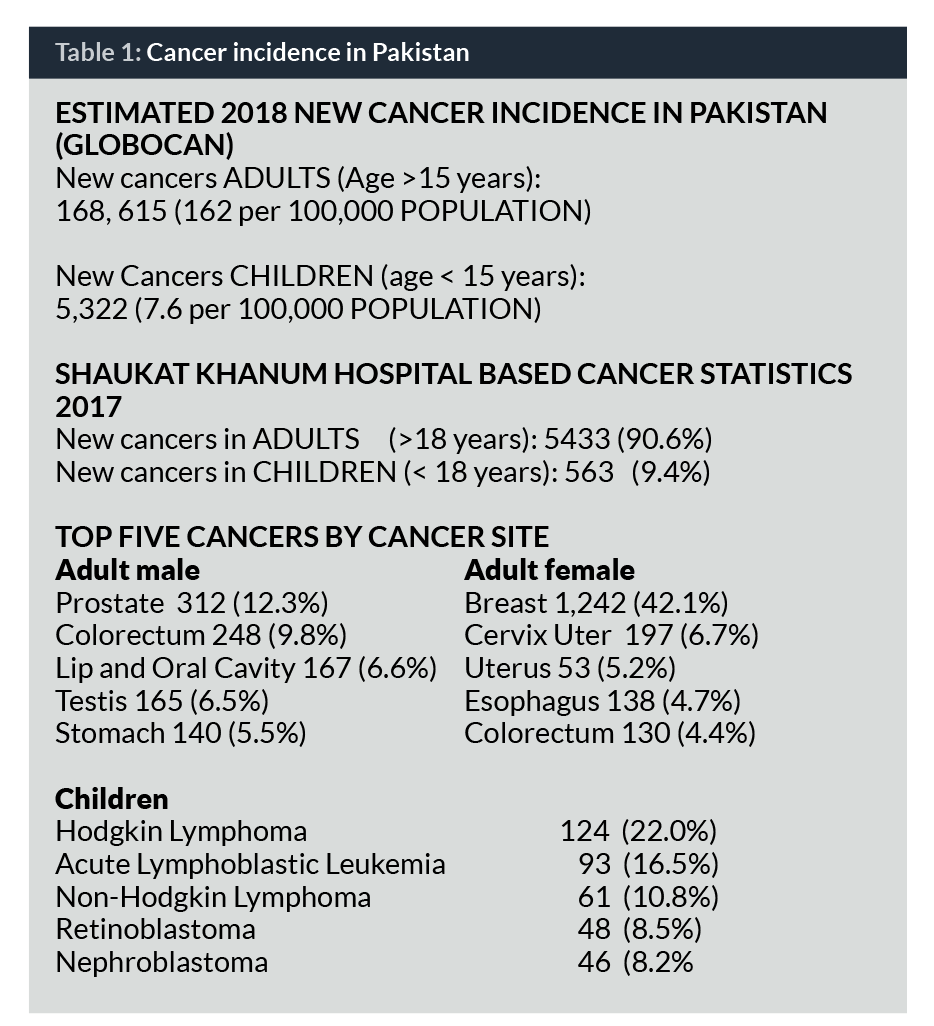
The most common cancers seen at the hospital are shown in Table 1. Since breast cancer is the most common cancer seen at the hospital, there are three specialized breast surgeons who also provide breast reconstructive services. Neurosurgery, gynaecology, ophthalmology, orthopaedics, head and neck surgery, thoracic and general oncologic surgery services are provided.
The number of outpatient visits and treatments given over the years are shown in Table 2.
Research
A fundamental concept of the hospital, enshrined in its name, is cancer research. As a fledgling institution this was difficult to start, but a major boost was given by the German Cancer Research Center (Deutsches Krebsforschungzentrum – DKFZ) in 1996. Under the leadership of Nobel prize-winner, Professor Zur Hausen, the DKFZ undertook to train our scientists and help in establishing our molecular and basic research laboratories. They have continued to collaborate with us, especially Professor Ute Haman, with the publication of a number of research papers.
Current status
The commonest cancers seen at the hospital are listed in order of frequency in Table 1, as well as the estimates for the country as a whole.
In 2017–2018, 72% of patients at the hospital were treated entirely free of charge. Another 13% received partially free treatment. Only 15% of patients bore the full cost of treatment.
On a daily basis, approximately 700 outpatients are seen at the Lahore hospital. Chemotherapy is given to an average of 130 patients daily (Table 2).
The future
The advent of the Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, has had a major impact in Pakistan, not only on clinical cancer services, but on hospital management, nursing services, pharmacy services and general health management. Regional health facilities have sent observers to the hospital and applied our hospital systems to their institutions. Nurses from these hospitals and pharmacists from other hospitals rotate through the SKMCH and return to their institutions to apply what they have learnt.
The hospital received recognition from the Joint Commission on 20 April 2018. It has been a long journey and it is continuing.
Because of the significant number of patients travelling from the north of the country and Afghanistan, in 2015, a new hospital with 250 beds was built and opened in the city of Peshawar, applying the same principles. This hospital currently provides diagnostic and chemotherapy services and will soon become a fully-fledged cancer hospital with surgical and radiation services.
A new hospital building has started in Karachi, the largest city in Pakistan, and is planned to open in 2021.
The Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, is now able to offer training in nursing, hospital administration and hospital pharmacy services to people from other countries. In addition, clinical attachments are available in various disciplines to medical students and doctors, with on-site accommodation (website: shaukatkhanum.org.pk).
It is our belief that with dedication and focus, and with public support, it is possible to build similar institutions in all developing countries and improve cancer care worldwide.
Biography